Full Name Age Gender Female Male Others Date of services Your phone Location Services Sample collection ECG Vaccination Tele consultation Write a Message Upload Prescription Consent Agree to terms & private policy Submit Full Name Age Gender Female Male Others Date of services Your phone Location Services Sample collection ECG Vaccination Tele consultation Write a Message Upload Prescription Consent Agree to terms & private policy Submit

 Book a Test
Book a Test
 Download Reports
Download Reports
 Health Packages
Health Packages
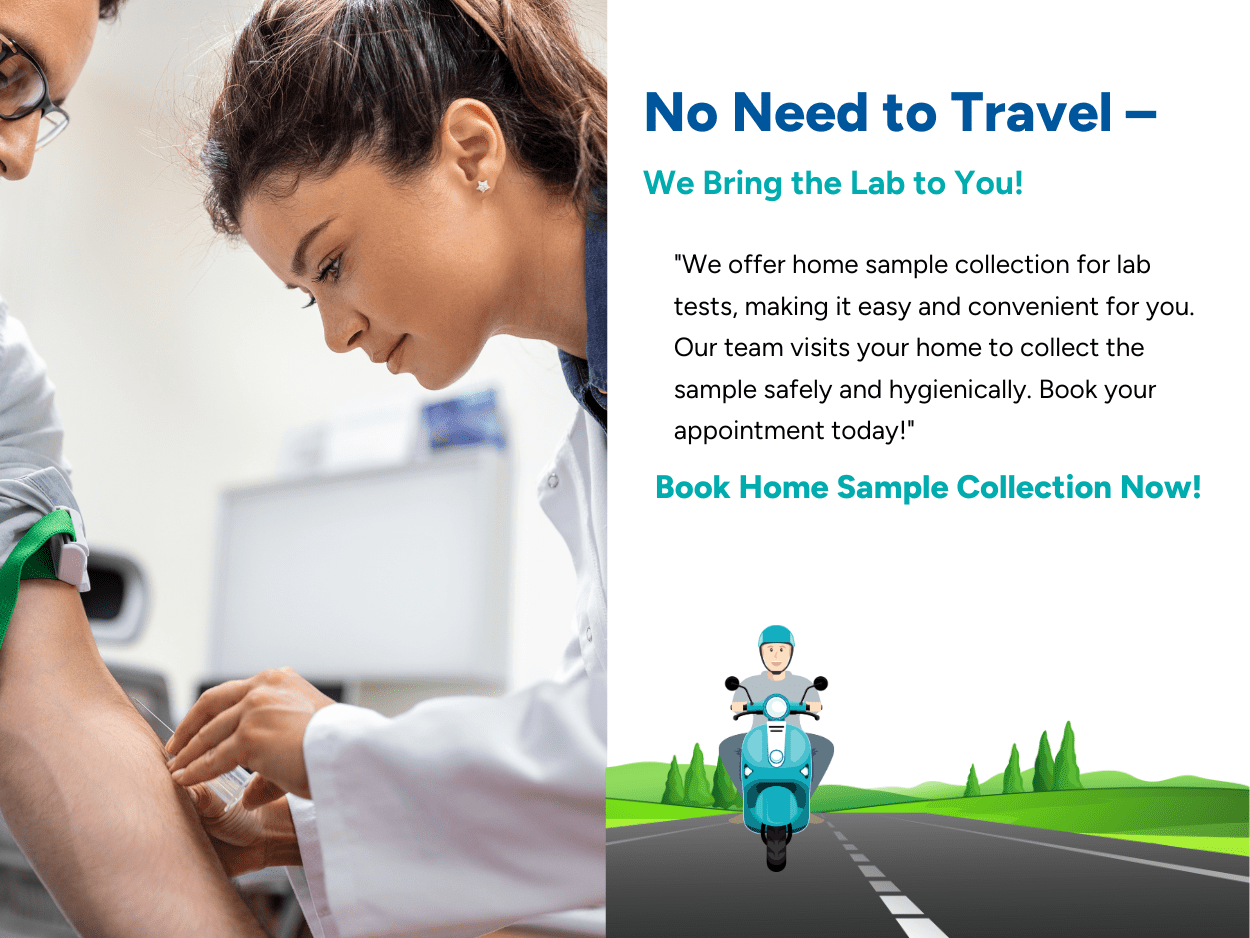
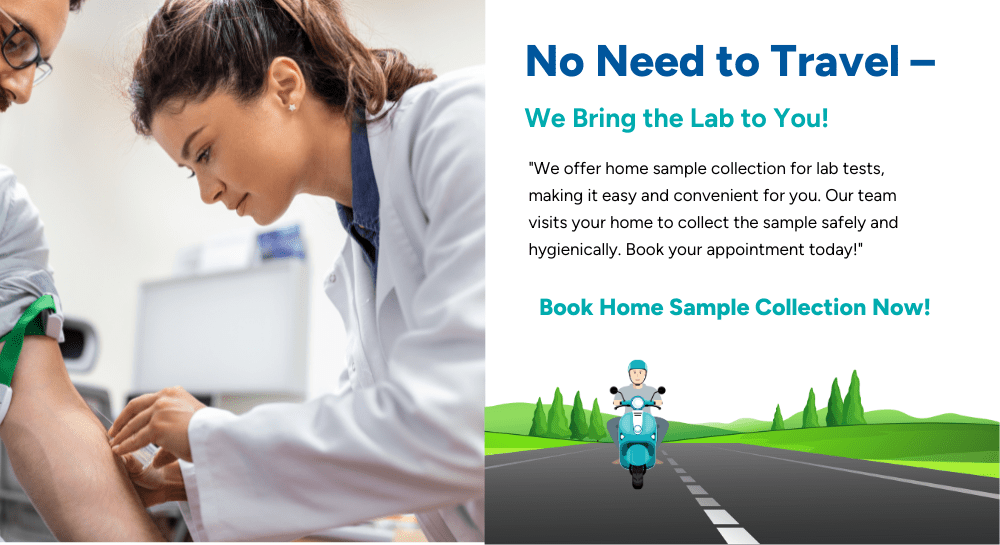
 Home Med Service
Home Med Service

